Why High LP(a) Overrides Statins — And the 3 Alternative Pathways to Protect Your Arteries
Why High LP(a) Overrides Statins — And the 3 Alternative Pathways to Protect Your Arteries
Written by: Lian Liu, MPH, RD, CDCES | Specializing in Cardiac & Menopause Nutrition. Reviewed and updated: June 2026.
> Direct Answer: Statins are ineffective against Lipoprotein(a) because LP(a) levels are genetically determined and utilize clearance pathways independent of standard cholesterol-lowering mechanisms. To protect your arteries, you must target risk through three specific pathways: PCSK9 inhibitors for direct LP(a) reduction, low-dose aspirin to manage clotting risks, and soluble fiber/plant sterols to drive your standard LDL to aggressively low targets.
Disclosure: Some of the links below are affiliate links. This means if you click through and take action, I may receive a small commission (at no extra cost to you). This helps support the free content on this blog while I only recommend tools and foods I truly believe in for your heart health journey.
When Jim had his heart attack, his doctor immediately put him on a high-intensity statin. Six months later, Jim’s standard lipid panel looked perfect: his LDL-C had dropped from 135 mg/dL to a stellar 62 mg/dL.
His doctor was thrilled. Jim felt relieved.
But a year later, during a routine cardiology follow-up, an ultrasound revealed that plaque was still accumulating in Jim’s carotid arteries.
"How is this possible?" Jim asked. "I take my pill every single night. My cholesterol numbers are right where you wanted them."
The answer lay in a test his doctor finally ordered: Lipoprotein(a). Jim's level was 195 nmol/L—placing him in the highest risk tier.
Jim’s story is incredibly common. Millions of cardiac patients take standard statin therapy every day, believing they are fully protected. But if you have high LP(a), standard statins leave a major gap in your defenses. In fact, statins do not lower LP(a) at all—and they can even cause a slight increase.
If you have elevated LP(a), you need to know why standard therapy is overriding your efforts, and the alternative pathways you must use to protect your blood vessels.
Why Standard Statins Can't Touch LP(a)
To understand why statins fail to lower LP(a), we have to look at how these drugs work.
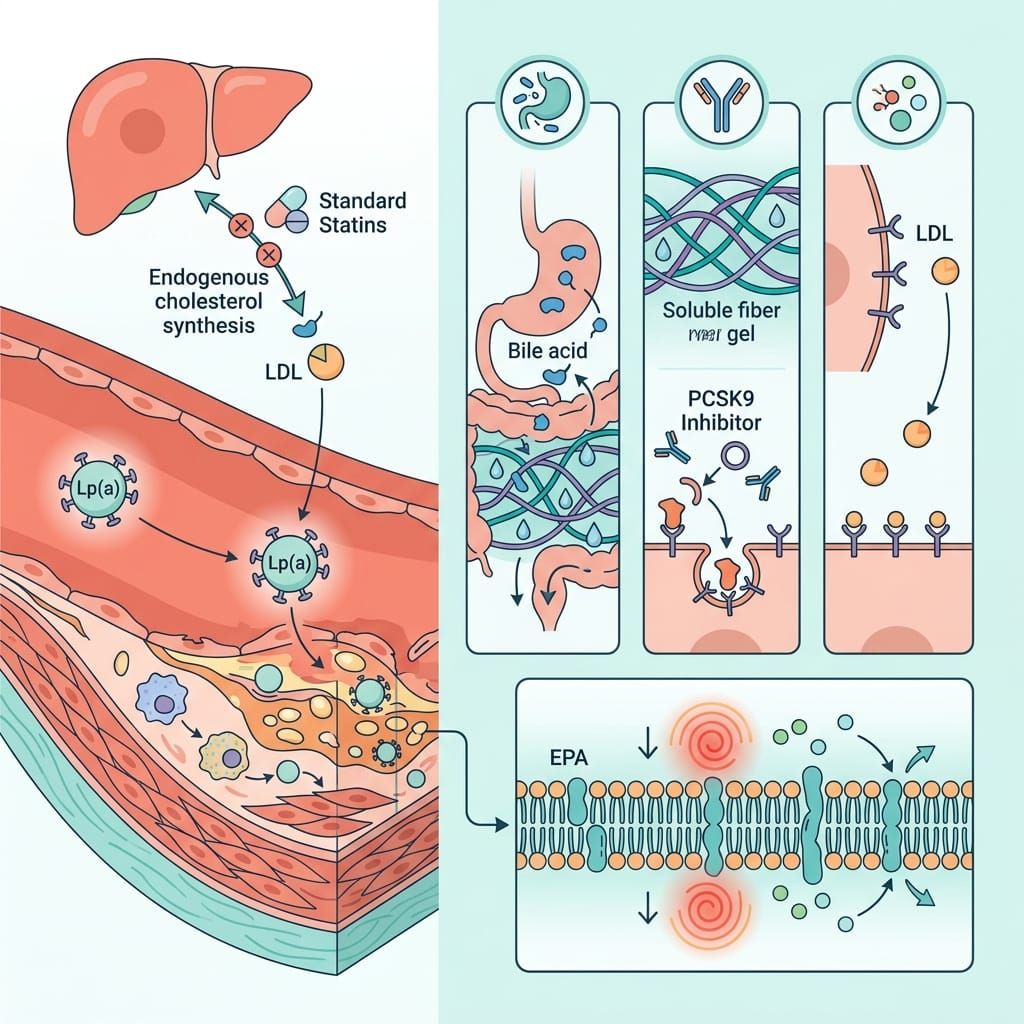
Statins block an enzyme in your liver (HMG-CoA reductase) that is responsible for producing cholesterol. When cholesterol production drops, your liver cells display more LDL receptors on their surface. These receptors grab standard LDL particles out of your blood and clear them away.
But LP(a) is different. It is a standard LDL particle that has a special protein called apolipoprotein(a) wrapped around it. This protein changes the particle's structure, preventing it from binding efficiently to standard LDL receptors.
The Clinical Paradox
Not only do statins fail to lower LP(a), but clinical data also demonstrates that statins do not meaningfully lower LP(a); average changes are small and may slightly increase in some analyses. A large systematic review and meta-analysis showed that statin use resulted in a minimal average increase of approximately 1.1 mg/dL (or 0.1% relative) in circulating LP(a) concentrations.
Crucial Safety Note: While average changes are small and can show minor elevations, clinical experts emphasize that this should never be a reason to stop taking your statin. Statins remain the bedrock of cardiac recovery. They drastically reduce your risk of a second heart event by driving standard LDL down, which stabilizes existing plaque. You should keep taking your statin, but recognize that it is only the first layer of your defense.
To fill the gap left by statins, you must target alternative pathways.
Pathway #1: The Advanced Lipid Clearance Route (PCSK9 Inhibitors)
Standard drugs like ezetimibe and bempedoic acid do not lower LP(a). However, a newer class of injectable medications called PCSK9 inhibitors (such as evolocumab and alirocumab) has been shown to lower circulating LP(a) by 20% to 30%.
How They Work
PCSK9 is a protein in your body that destroys LDL receptors. By blocking this protein, PCSK9 inhibitors allow your liver to keep thousands of extra LDL receptors active on its surface. Even though LP(a) binds poorly to these receptors, the sheer volume of active receptors is so high that they manage to pull a significant amount of LP(a) out of circulation.
Clinical Impact
Data shows that high-risk cardiac patients with elevated LP(a) derive an even greater cardiovascular benefit from PCSK9 inhibitors than patients with normal LP(a) levels. Landmark studies on evolocumab reveal significant risk reductions for these patients, and a pooled analysis of alirocumab trials demonstrated a corresponding decrease in major adverse cardiovascular events. If your LP(a) is high and your standard LDL-C remains ≥70 mg/dL on maximally tolerated statin therapy, the National Lipid Association (NLA) recommends that your doctor consider adding ezetimibe or a PCSK9 inhibitor to intensify your treatment.
Pathway #2: The Anti-Clotting Defense (Low-Dose Aspirin)
LP(a) does not just contribute to plaque buildup; it is also highly prothrombotic (promotes blood clotting).
The structure of the apolipoprotein(a) on LP(a) is nearly identical to plasminogen, a protein your body uses to dissolve blood clots. Because of this similarity, LP(a) binds to clotting sites and blocks your body's natural ability to dissolve clots. This makes a sudden, clot-induced event (like a heart attack or stroke) much more likely if a plaque ruptures.
The Role of Aspirin
Because of this high clotting risk, guidelines recommend that patients with elevated LP(a) have a risk-benefit discussion with their doctor about using low-dose aspirin (81 mg) for cardiovascular prevention.
While aspirin carries a minor risk of bleeding, patients with elevated genetic LP(a) levels are far more likely to experience protective benefits from daily anti-platelet therapy than the general public.
Pathway #3: Aggressive Particle Reduction (Additive Nutrition)
Since we cannot easily lower the genetic LP(a) particle itself, we must focus on reducing standard LDL particles to the absolute minimum. Think of it as clearing the roadway of all normal cars so the sticky genetic trucks have nothing to collide with.
Strict Targets
For patients with elevated genetic cardiac risk, modern preventive guidelines advocate for a strict "lower is better" target:
- LDL-C Target: Keep LDL-C <55 mg/dL (and <40 mg/dL if subclinical arterial plaque is already present).
To hit these aggressive goals, you can layer nutritional interventions on top of your medical therapy:
1. Viscous Soluble Fiber
Consuming 10 grams of viscous soluble fiber (like psyllium, oats, and barley) daily has been shown to lower LDL-C by an additional 5% to 10%. Soluble fiber forms a gel in your gut that binds to bile acids (which are made of cholesterol), forcing your body to excrete them and use circulating LDL to make new ones.
- Lian's Tip: Adding a daily scoop of Metamucil Sugar-Free Psyllium Fiber is the easiest way to hit this target with zero friction.
2. Plant Sterols and Stanols
Consuming 2 to 3 grams of plant sterols or stanols daily can lower LDL-C by 9% to 20% by blocking cholesterol absorption in the digestive tract.
3. Vessel-Protecting Omega-3s
To further protect your endothelial walls from the inflammatory damage caused by high LP(a), focus on high-dose prescription purified EPA (icosapent ethyl). The landmark REDUCE-IT trial demonstrated that taking 4g/day of purified EPA reduced major adverse cardiovascular events by 25% in high-risk patients.
- Lian's Tip: If you do not consume fatty fish regularly, you should consider a practitioner-grade, third-party tested Omega-3 supplement. You can browse my vetted, clinical-strength formulations at a discount in my Fullscript Dispensary.
The Horizon: Emerging Gene-Silencing Therapies
If you are frustrated that current options only lower LP(a) by 20% to 30%, there is major hope on the horizon. Multiple pharmaceutical trials are currently evaluating gene-silencing therapies that target the LPA gene directly in the liver:
| Therapy | Mechanism | LP(a) Reduction | Clinical Trial Phase |
|---|---|---|---|
| Pelacarsen | Antisense Oligonucleotide (ASO) | >80% | Phase III (Lp(a)HORIZON) |
| Olpasiran | Small Interfering RNA (siRNA) | ~100% | Phase III (OCEAN(a)-Outcomes) |
| Lepodisiran | Small Interfering RNA (siRNA) | 94% (sustained) | Phase III Enrolled |
| Muvalaplin | Daily Oral Pill (disrupts synthesis) | Pending | Phase II |
These therapies will likely change the standard of care over the next few years. Until they are FDA-approved and widely available, utilizing the three alternative pathways detailed above is your most powerful tool to protect your heart.
Your Action Step
If you know your LP(a) is elevated, do not wait for the future gene therapies to protect you. Take action today:
- Schedule a Discussion: Call your doctor or cardiologist and ask: "Since my LP(a) is high, are we targeting an LDL-C of <55 mg/dL? Should we consider adding a PCSK9 inhibitor or low-dose aspirin?"
- Add Soluble Fiber: Start adding 10g of soluble fiber to your daily routine (using a supplement like Metamucil or adding ground flaxseeds and oats to breakfast).
Taking control of your pathways means you are no longer at the mercy of your genetics.
For the complete blueprint to rebuilding your diet, controlling inflammation, and navigating cardiovascular recovery, pick up your copy of The Cardiac Comeback.
Stay Ahead of Your Heart Health
Want to stay up-to-date with current science-backed nutrition tips to protect your cardiovascular future?
- Subscribe to the Newsletter: Get practical, clinical-strength tips on diet, labs, and lifestyle adjustments sent straight to your inbox.
- Get the Master Course: Secure immediate access to the Heart Disease Risk Reversal Master Course and start reversing your risk today.
👉 Join the Newsletter & Master Course here
Keep moving forward.

Download Vetted Clinical Handouts & Trackers
Get instant access to a growing library of evidence-based guides, food protocols, and symptom logs vetted by a cardiology dietitian. Access is completely free—simply subscribe to view.
Access Handout Library




Member discussion